
“Syndrome: A group of symptoms or pathological signs which consistently group together, esp. with an (originally) unknown cause; A characteristic combination of opinions, behavior, features, social factors, etc.” – Oxford English Dictionary
According to a wide range of experts interviewed for this investigation, the rise in the breast cancer incidence rate that began more than three decades ago among affluent white women in Marin County does not signify the presence of a cancer cluster.
Nor do places with similar demographics and historically high incidence rates, such as Cape Cod, Long Island, Seattle and southern Orange County, represent clusters. Rather, these areas cast statistical mirages resulting from access to state-of-the-art health care.
The explanation is simple. The more screening mammograms, clinical exams and biopsies a woman gets, the more likely she is to be diagnosed or overdiagnosed with breast cancer. And the results are entered into the California Cancer Registry.
The media has treated the so-called Marin cancer cluster as a real and present danger for decades, generating social anxiety and a misallocation of public resources. Chief among the scientific sources cited in the news is the Cancer Prevention Institute of California, formerly called the Northern California Cancer Center.
Since the late 1980s, the institute has operated the Greater Bay Area arm of the California Cancer Registry, summarizing medical records for cancer cases for inclusion in a statewide database.
Based on the registry data it collects, the institute has long claimed that women in Marin suffer from an excess of breast cancer whose causes are largely unknown.
The institute’s board of trustees includes socialites, high-tech business people, lawyers and medical professionals. Its chair is private-equity investor Samuel Bronfman II, of the Seagram & Sons, Inc. liquor and chemicals fortune. Gap founder Doris Fisher sits on the board, as does Hilary Newsom Callan, president of the PlumpJack Management Group, which sells high-end wine, liquor and food services in Northern California.
The institute’s “partners” include Chevron, Genentech and Goldman Sachs Group.
Its $18.8 million budget is funded by the National Cancer Institute, the Centers for Disease Control and the California Department of Public Health. Other assistance comes from Safeway Foundation, the United States Department of Defense and an annual golf tournament sponsored by PlumpJack.
The institute’s official mission is to “stop cancer before it starts” while educating the “under-served” public about “cancer-related issues.” Toward that end, it pays nearly $1 million a year to rent a suite of offices in suburban Fremont. One percent of the budget is slated for “education.” The balance of the budget supports cancer registry data-gathering operations, the research of a dozen scientists, and two public relations specialists.
The registry
State law requires that hospitals, laboratories and physicians report cancer diagnoses and treatments to the 10 regional arms of the California Cancer Registry within six months of discovery. Data on individual cases is supposed to be checked for accuracy at the local level, then transmitted to a central data bank currently overseen by the University of California, Davis Health System.
Registry statisticians calculate local, regional and statewide cancer incidence rates that are used by public health agencies to guide funding priorities. Since the registry’s inception in 1988, the data it collects has fueled hundreds of studies into correlations between cancers and possible causes.
But, according to data quality audits obtained by the Light, it is difficult for the registry to verify the completeness and accuracy of its sprawling information network, which includes data submitted late by thousands of hospitals, doctors’ offices and pathology labs.
Due to persistent software and medical-record coding problems, high rates of clerical errors and an absence of follow-up on previously reported cases, the registry’s breast cancer incidence numbers are inflated by duplicate cases, false positives and overdiagnoses.
In fact, the registry’s data is of such questionable quality that a study co-authored by experts from the University of California, Los Angeles and published in Journal of the National Cancer Institute in 2002 warned, “Reporting the quality of care derived from [California Cancer Registry] data with such validity problems could anger providers and seriously undermine public confidence in this process.”
Since the publication of that study, the quality of registry data has further deteriorated, public records show.
These deficiencies, combined with the fact that the women with the highest breast cancer incidence rates are also those getting the most cancer screening, explain what we shall call the “Marin Syndrome”: the endless search for the cause of a non-existent epidemic.
The Marin Syndrome
According to an in-depth investigation conducted by the Centers for Disease Control in the late 1990s, the higher-than-average use of mammography by affluent white women in the Bay Area accounted for that population’s elevated breast cancer incidence rates.
At the time, local public health officials and breast cancer activists emphatically discounted the agency’s report as biased.
The C.D.C.’s critique of research published by the Cancer Prevention Institute of California was popularly dismissed as politically motivated, and the San Francisco Chronicle led the local media in treating the Marin breast cancer cluster as scientifically unassailable.
Christina Clarke, Sally Glaser and Dee West are the institute’s leading breast cancer epidemiologists. In 2002, along with Rochelle Ereman, the chief epidemiologist at Marin Health and Human Services, they proclaimed in a widely publicized study of non-Hispanic white women that Marin’s high breast cancer incidence rate is a “canary in the gold mine.” The scientists speculated that educated, affluent women are more susceptible to breast cancer due to lifestyle choices.
Lacking any hard evidence of causation, they tagged the most likely culprits as excessive alcohol use, higher-than-average use of hormone replacement therapy and not bearing children. They explicitly excluded environmental factors and the quality of cancer registry data as explanatory of the strangely elevated rates.
Importantly, they remarked that while high breast cancer incidence rates for affluent women could be an artifact of greater-than-average screening rates, there is “no evidence of substantially elevated rates of mammography utilization [in] Marin County.”
But according to the California Health Interview Survey, a biannual survey conducted by the University of California, Los Angeles, wealthy white women in Marin have been getting substantially more mammograms than women of all other races and income levels throughout California since the first survey was taken in 2001.
As we shall learn next week, the “gold mine” paper’s inflated incidence claims were later corrected to reflect much lower rates.
An uncertain science
Epidemiology is not an exact science. Using the limited information provided by incidence rate trends, it tries to track the path of diseases through large populations, while hypothesizing possible causes of changing rates.
It is important to remember that cancer incidence rates are not identical to the actual number of newly diagnosed cancers reported. Rather, they are extrapolated from real counts to permit comparisons of demographically different populations.
A more meaningful measure of a population’s cancer burden is mortality rate. (Marin’s has long been flat.) Unfortunately, mortality rates are difficult for state-based registries to track, since patients move to other states, change medical providers or die from other causes. So the reliability of cancer epidemiology remains dependent upon population-based data that is cratered with data deficiencies.
During the last quarter-century, scientists have shown that breast cancer incidence rates in a given population track the rise and fall of breast cancer screening rates. This may seem obvious, but popular belief incorrectly regards incidence rates as a measure of the amount of breast cancer in a population and the risk of getting the disease.
Incidence rates can be useful for comparing the rate or frequency with which various populations experience a disease over long periods of time—after accounting for factors that can disguise the virility of a disease, such as differences in age or access to health insurance.
Epidemiology recognizes that sharp spikes in incidence rates can indicate “patient zero” locations for infectious diseases like cholera and measles. But identifying a contributing cause of an outbreak of disease (such as drinking water sourced near a latrine or being sneezed upon by a measles-infested Mouse at Disneyland) requires on-the-ground investigation. Causation cannot usually be identified by purely statistical analysis.
Incidence rates are not particularly useful tools for investigating the causes of chronic diseases like cancer because any set of cases has multiple, interacting causes that are mostly untraceable over patients’ lifetimes.
Nonetheless, some cancer epidemiologists incorrectly frame incidence rates as reflections of personal risk factors, possibly to justify their jobs to the inexpert public.
What would it take for incidence rates to pinpoint a real cancer cluster? If the disparity in breast cancer incidence rates between Marin and a comparable population numbered in the hundreds of new cases, that might indicate a cluster.
But the Marin differential is counted in single and low double digits, which are statistically insignificant in terms of absolute risk.
If breast cancer mortality rates in Marin had shot up disproportionally over the years, that would also indicate a real problem. But those rates have remained flat or in decline.
The Light discussed the Marin situation with Boston University professor Kenneth Rothman, one of the most respected figures in epidemiology.
“I would not call it an epidemic, nor do I believe many epidemiologists would,” he said. Just as this investigation found, Dr. Rothman attributed Marin’s elevated incidence rates to the high use of mammography.
Who gets mammograms?
It is well documented that in California, women with higher incomes get significantly more mammograms than do poorer women. In 1997, the California Department of Public Health published a pamphlet reporting that 72 percent of insured women and only 44 percent of uninsured women received a mammogram in the previous year. In 2004, Marin Health and Human Services reported that 70 percent of insured women in Marin got regular mammograms, versus only 27 percent of uninsured women. Kaiser Permanente has reported that 90 percent of women over age 50 in Marin whom it insures get mammograms at least every two years.
The American Cancer Society assesses that nationwide, only one third of uninsured middle-aged women get regular mammograms, whereas 71 percent of insured middle-aged women do. Clearly, access to insurance tracks access to mammography, which also tracks the rise and fall of incidence rates (and overdiagnosis).
Every two years, researchers at the University of California, Los Angeles administer the California Health Interview Survey by randomly dialing landlines in all 58 counties. Interviewers ask adults a range of health-related questions, including the frequency with which they get mammograms. The self-reported survey data can track basic trends.
In 2001, according to the survey, all women living in Marin received 7 percentage points more mammograms than did all women living in California—66 percent compared to 59 percent. A paper authored by Cancer Prevention Institute of California researchers acknowledged that this screening excess was “significant,” but the authors declined to investigate the impact of the excess on incidence rates.
Ten years later, the Marin-California mammography gap for all women had widened by 8 percentage points.
The mammography utilization gap increases when stratifying the survey data by race, age and income. Marin is white and old: the most recent United States census records Marin as 72 percent white and 16 percent Latino, with smaller black and Asian populations.
In 2012, white women in Marin got 16 percentage points more mammograms that did all white Californians. Compared to other counties in California, Marin has a disproportionately large population of white women over 50; it also has the highest life-expectancy rate of all counties in the United States—an obvious sign of a health-conscious population.
As we learned in the last part of this series, aging accounts for 80 percent of breast cancer risk, and older women get more mammograms than do younger women. From 2001 to 2012, X-ray screening in Marin shot up by a third, and incidence rates climbed.
According to state health department reports, Marin’s excess incidence is primarily composed of “early-stage” cancers, which are only found by mammography and are often overdiagnosed.
Malignant breast cancers can take decades to evolve. Our bodies contain pools of extant and potential cancer cells; some remain dormant, some are slated to regress, some are fated to metastasize and kill the host.
It is not surprising that Marin’s invasive breast cancer rates, which were ascending, are now trending toward decline. The population’s collective pool of existing cancers and cellular abnormalities is likely diminishing due to decades of what is called “screening saturation.” (When first introduced, mammography causes a spike in incidence rates that collapses as the population is thoroughly screened.)
Marin differs from most counties in California because it is rich. Marin’s median family income is $90,000, meaning that half the families make more than that. The statewide median family income is $61,000.
(Our investigation defines low-income as a family of four making less than $24, 250, the federal poverty level, and high-income as four times the poverty level, or more than $97,000.)
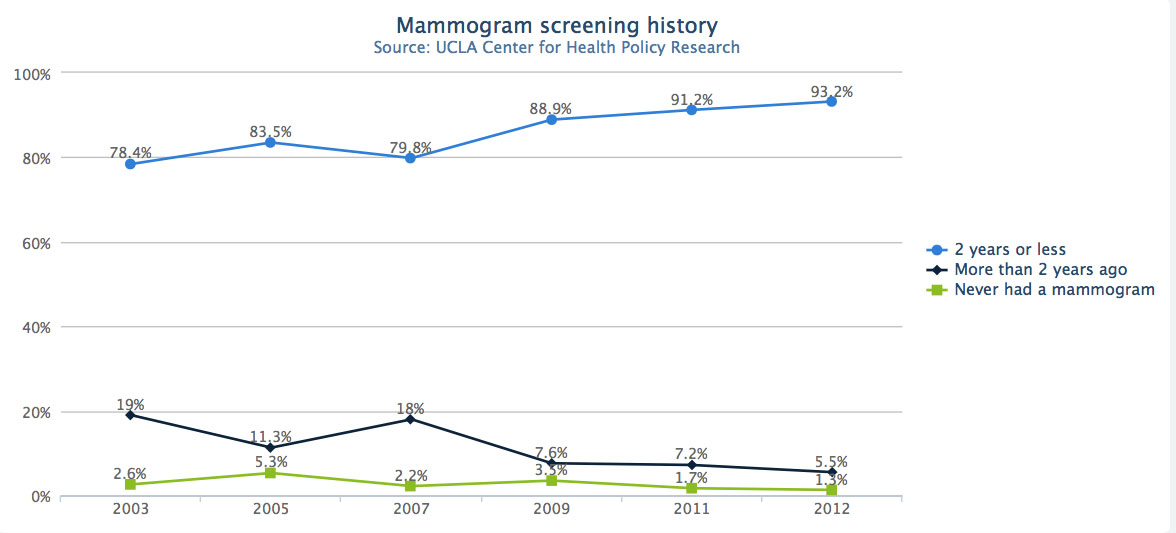
Remarkably, the 2012 California Health Interview Survey estimated that 93 percent of high-income white women in Marin between age 40 and 74 got mammograms every two years or less. For middle-aged, low-income women of all races in California, that number was 70 percent.
That means that wealthy white women in Marin received a third more mammograms than less wealthy Californians in this age range.
Tellingly, wealthy Marin women received 6 percentage points more mammograms than their high-income counterparts throughout the state. And high-income white women of all ages in Marin got 34 percentage points more mammograms than the average Latina or Asian Californian.
Robert Hiatt chairs the Department of Epidemiology and Biostatistics at the University of California, San Francisco. He studies the fine tunings of breast cancer risk: the possible carcinogenicity of estrogen-producing reproductive behaviors combined with genetic predispositions and exposures to household chemicals.
In an interview with the Light, Dr. Hiatt said that lifestyle and genetic factors do not have much “explanatory strength” in accounting for historical fluctuations in Marin’s breast cancer incidence rates.
He also agreed that overdiagnosis could account for elevated incidence rates in Marin.
An entrenched conviction
A 2005 brochure published by Marin Health and Human Services and Zero Breast Cancer, a Novato-based nonprofit, bluntly stated that “high socio-economic status makes women at high risk for breast cancer” because of lifestyle factors. Conversely, the authors stated that highly educated Marin women have a higher-than-average practice of protective factors, such as breastfeeding, exercising and healthy diets. Finally, they claimed that the increase in breast cancer incidence was not due to screening, because “the data do not show evidence of an increase in the proportion of cancers diagnosed as in situ over time.”
The logic of that last statement is correct. If greater screening led to greater breast cancer incidence rates, the rate of diagnosis of ductal carcinoma in situ, or D.C.I.S., would increase more rapidly than that of invasive breast cancer.
But the fact is cancer registry data do show a steady annual increase in the proportion of D.C.I.S. diagnoses to invasive cancer diagnoses since the registry’s inception. The 32 cases of D.C.I.S. recorded for Marin in 1988 rose steadily to 94 cases in 2009. The proportion of D.C.I.S. to invasive cases in 1988 was 16 percent, more than doubling to 36 percent in 2009.
Asked why the county had published an untrue statement about the D.C.I.S. data, county epidemiologists and Public Health Officer Matt Willis declined to comment.
The Marin Syndrome has socio-political consequences. Scores of national studies show that screening rates drop precipitously as incomes fall. Poorer women living in Bay Area communities with highly toxic environments such as Richmond, Vallejo or Bayview-Hunters Point obtain far fewer mammograms than do Marinites. As a result, they are tagged with lower incidence rates.
Lower-income women also receive inferior treatment for breast cancer due to a lack of decent health insurance, enormously impacting their mortality rates. The breast cancer mortality rate for black women in California is a third higher than for whites, despite black women having lower incidence rates than white women, according to the cancer registry.
In conclusion, Marin County public health officials and the Cancer Prevention Institute insist that breast cancer has preferentially attacked white women in Marin despite plenty of evidence that high incidence rates are explained by high screening rates.
In an interview with the Light, Stanford epidemiologist Alice Whittemore summed up the ongoing harm caused by the Marin Syndrome: “I am amazed that millions of dollars continue to be spent studying this issue. This is not a scientific question, but rather a social and psychological one. It concerns the level of evidence that is needed to dislodge an entrenched conviction, albeit one vested with potent emotional force. How you convince people that their irrational fear is not grounded in good data?”
Next week’s serial tackles the politicization of the claim that wealthy white women are most at risk of breast cancer, despite the fact that poor women of color die from it more often.
This article was amended on Dec. 1 to clarify several sentences discussing percentage differences.
Read Peter Byrne’s investigative series on a nationwide breast cancer scare that never should have happened:
- Part 1: René Willard’s story
- Part 2: Climbing Risk Mountain
- Part 3: The Marin Syndrome
- Part 4: The canary in the gold mine
- Part 5: Does hormone replacement therapy cause breast cancer?
- Part 6: The perils of mammography
- Part 7: The life and death of the Marin Women’s Study
- Part 8: How Zero Breast Cancer pays its bills
- Part 9: Bad Data: The Dirty Laundry
- Part 10: Bad Data: Audit Trail
- Part 11: The story of Abigail Adams: How the California Cancer Registry fails women