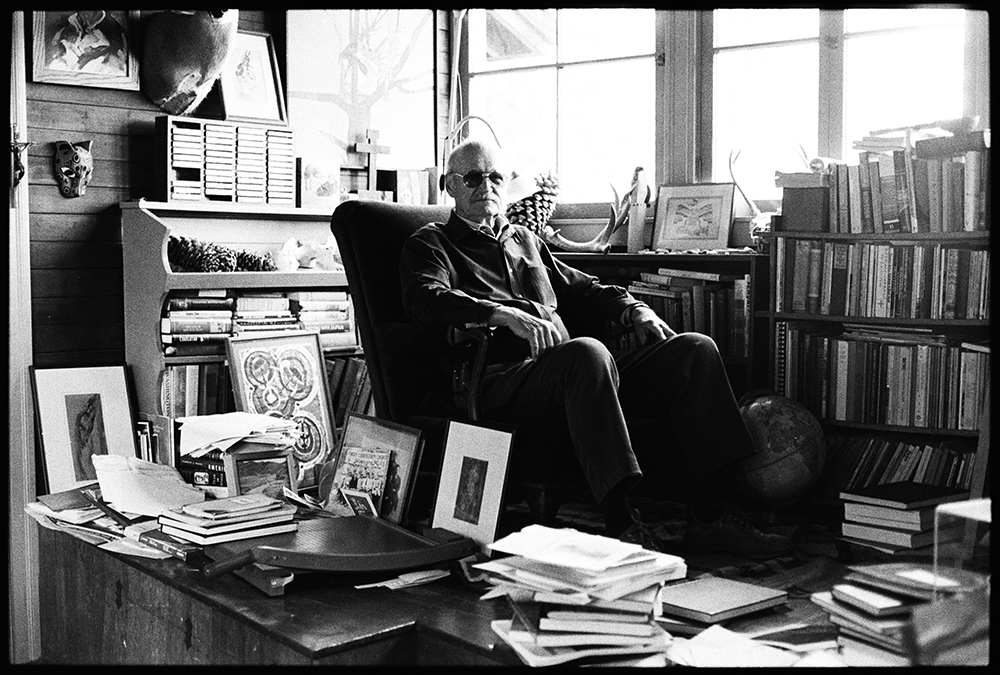
Dr. Michael Whitt, a Texas native who forsook a career in petroleum engineering to study medicine, served countless families during his four decades as West Marin’s primary care doctor before he retired in January. General medicine was not always the focus of his practice: in the 1970s, soon after he answered a “Doctor wanted” ad posted in Point Reyes Station, he and his colleagues devoted much of their time to home birth. They delivered close…
Michael Whitt: A life in country medicine